Paddison Program Disclaimer: This podcast does not constitute medical advice. All changes for any medications, diet, and exercise should be made in consultation with a professional who can assist your unique health circumstances.
In Episode 17 we welcome back author of the ‘The Symbiont Factor‘ and Richard Matthews so we can learn about Hormones and Rheumatoid Arthritis:
– How gut bacteria influence autoimmune conditions like RA and psoriatic arthritis (and many more)
– How gut bacteria interact with hormones
– Why women can go into remission for RA during pregnancy
– Why pain comes back quickly after giving birth
– How monthly female cycles can affect pain levels
– Could hormone therapy be good at relieving Rheumatoid Arthritis symptoms?
[powerpress]
Clint Paddison: Welcome back to the Paddison Podcast. Today, we are very happy to welcome back Dr. Richard Matthews, the author of The Symbiont Factor. It’s our third time to have him on an episode and today, we want to ask Richard all about hormones and rheumatoid arthritis. Welcome back, Richard.
Dr. Richard Matthews: Thank you. Thank you, Clint. I’m happy to be here.
Clint Paddison: So we’ve got you back. You’re an expert of many things, and the one thing that we keep asking you all about is regarding gut bacteria. And there is a massive amount of scientific evidence to support a relationship between gut bacteria and autoimmune conditions. So we have covered a lot of this in the past two episodes, but for those people who may have missed those two episodes or just want a refresher before we talk about hormones and their effect on rheumatoid arthritis, and the way that that’s influenced by gut bacteria, perhaps if you could just give us a little bit of a bird’s-eye view again, and a recap on why we should be talking about gut bacteria if we have an autoimmune disease.
Dr. Richard Matthews: Okay, very good. Thank you, Clint. The connection is that early in life when we’re born, our immune system is what we would call naive. It hasn’t really seen anything but our own tissue. And the gut bacteria that populate our intestines interact with our nervous system and with our immune system and essentially, they act as the nanny and the first teacher of the immune system. They basically teach the immune system what to react to and what not to react to. If you were to consider your immune system a military, you would say an autoimmune problem is like friendly fire casualties. It should’ve been looking outside the gates, as it were, at perhaps invading infectious agents, bacteria, but instead, it reacted to something in the body.
Now one of the biggest sources of data on that is research supporting what is known as the Hygiene Theory. And hygiene theory is very simply the observation that people that live in modern, industrialized countries where we sanitize everything, we disinfect a baby when he’s born, when she’s born, they’re born in hospitals where we try to disinfect everything as much as possible, and mom uses sanitary baby wipes, everything is sprayed down with bleach and so forth, we’ve done that for years with the thought that we’re doing some good protecting baby from infection when, in fact, we’ve gone so far with it that we’ve protected baby from any invading organisms that might have helped baby’s immune system learn what it’s there for.
The observation is that in other countries perhaps Third World countries, granted they may have other health issues, but they tend to have little to no autoimmune problems and that contrast is called Hygiene Theory. In my book, I contrast it with what I call the “Farm Effect,” which is the observation that people that live on farms, children that grow up on farms or have pets, are exposed to a certain degree of natural filth and that seems to have a therapeutic effect. I essentially call it “target practice for the developing immune system” so that the troops know how to aim. Otherwise, they end up having friendly fire incidents and start reacting to your joints, or your thyroid, or parts of your own body in any case.
The gut bacteria themselves show the immune system how to work and they interact with dendritic fibres that are nerve endings that go down into the gut, and those are intimately related to the production of the actual immune reactive factors that white blood cells produce. There’s a very, very special dance, if you will, that happens between the host, the immune system, and the bacteria and sometimes even other organisms that may end up in the mix.
The goal when everything works is that the immune system can tell the difference between what’s dangerous and what’s not, and it knows when to react and when not to. That’s optimum. When it goes out of balance, it will go one of two ways. It will either not react to something that it should have. An example of that would be the development of cancer where the immune system should’ve recognized that and it killed it, but it overlooks it that time. Or the opposite extreme, where it reacts to things that it should not react to like your synovial cartilage, synovial tissue in your joints.
Now, a lot of that really comes down to how the gut bacteria develop. The most recent research shows that a newborn baby has a primitive microbiome already installed and transported as a minimal subset from the mothers. So babies aren’t completely sterile before they even start birth. They have some microbiome but the biggest dose of starter culture happens from vaginal birth. Babies that are born through C-section start out with a lot less normal bacteria and their microbiome resembles a bit more of what you would normally see on skin, because that’s the only thing that’s really exposed to skin, mom’s skin and maybe skin of other people that handle the baby. But the initial starter culture normally is from vaginal birth and then it’s added to by breast-feeding.
Clint Paddison: Right. So someone who’s had a vaginal birth, the bacteria comes into the orifices, doesn’t it, through the eyes, through the nose, through their mouth, through the baby, and that’s how that initially creates this starter. Is that right, through their orifices?
Dr. Richard Matthews: Absolutely, absolutely. It’s like a big batch of natural probiotic really.
Clint Paddison: Yes. And then, of course, if someone’s had a C-section and they then put their baby on formula, then the baby is very, very deficient in this gut bacteria for quite a long period of time.
Dr. Richard Matthews: Right. And there’s several stages where that can be affected, and it’s best to look at them as perhaps risk factors. And if you know you’re going to have one, you might try to limit another. The initial bacteria that the baby gets before it even begins the birth process, we know that because it shows up in their first bowel movement, meconium, that bacteria is strongly affected by the mother’s experiences during pregnancy. If she’s under a great deal of stress, that will cause that gut bacteria to be a bit more imbalanced.
Let’s say, if the mother is on antibiotics, that will cause some diversity in the initial, and then there’s the method of birth, which unfortunately a mother may not always have a choice. I don’t know how many would actually choose a C-section, but then the third part is, of course, breast-feeding versus bottle feeding. So with my own patients that have been through childbirth, if they know they’re going to have to have a C-section or something went wrong, and they ended up having to have a C-section at the last minute, some of that damage can still be mitigated if they will breast-feed afterward. But then if a mom has a stressful birth and a C-section and bottle feeds, you’ve combined really three negative things all in one place and that raises the odds of there being problems, let’s say.
Clint Paddison: Okay. Well, it’s very fascinating stuff, and you and I can talk about these things and I’m sure our listener enjoys these things. We could continue to talk about that, on that path for a lot longer, but let’s get back on track. And I just want to summarize just the initial reminder to us about the importance of gut bacteria and autoimmune conditions with this simple question. On a scale of 1 to 10 with one being almost nothing and 10 being absolutely the highest factor, what score would you say that gut bacteria have on an autoimmune health?
Dr. Richard Matthews: I would say that’s probably 9 or 10, because it’s hard to think of anything else that would affect it more so.
Clint Paddison: Good, that’s what I wanted to hear. That’s what I wanted you to say. I think that that sets the platform for us every time we chat and for people to be reminded by the importance of feeding and providing a healthy environment for the gut bacteria as an upmost importance so that they can have the most well-behaving and manageable immune system.
Let’s now move on to talking about the title of this conversation, which is hormones and rheumatoid arthritis. And I’ll lead into this by talking about lots of emails that I get and also correspondence that I have where I personally coach and help people on our online forum who describe the situation…particularly two situations where they notice the most influence of hormones and their RA. Of course, these are females because these two situations are as follows.
Firstly, during pregnancy. It seems to be fairly well accepted that maybe 60 or 70% or thereabouts of females who fall pregnant tend to have a significant drop in the rheumatoid symptoms during pregnancy and then the pain all comes back after the baby is born. And then secondly during monthly cycle. A lot of women will talk about a flair or reaction that they have that is really spiked around the time of their monthly cycle.
And because I get these questions all the time, and it’s something that a lot of people are concerned about, I wanted to ask for your help and guidance and for an explanation as to what’s going on so that once we have an understanding of what’s going on, it takes all of the sting and all of the worry and all of the concern out of it, and we feel more empowered. So let’s start with talking about the steps to which those instances through a woman’s life can affect inflammation. Perhaps you can walk us through and get us to an understanding of how the inflammation can be affected by those two periods of a woman’s life?
Dr. Richard Matthews: Absolutely, I’d be glad to. The simplest way to understand it is to think about what a woman’s body is trying to prepare for, pregnancy and childbirth. So in general, in order to sustain a pregnancy, the mother’s immune system has to have some shore leave and lowered a DEFCON 2, if you will, and not be on alert so much.
Because otherwise, the immune system could easily regard a new baby as a tumour, as an invading organism, which in fact, it kind of is. It doesn’t even have…only 50% of the DNA matches so since the immune system is to some extent keyed to your individual…to the mom’s individual DNA, the immune system has to be tuned down a little bit in order to tolerate pregnancy and prevent miscarriages. So right off the bat, we know that that has to happen some.
The second aspect is as a woman gets closer…as a pregnancy gets to the time of delivery, that is…I was blessed to watch all three of my children born, and I’m still in shock and amazement at what a woman’s body can actually do, and recover and not just go into an extreme state of shock. And part of that is again, because the immune system is told, “Listen, something crazy is about to happen, don’t go nuts with the inflammatory response.” Because if you think about what normally would trigger inflammation and then you look at the birth process, it should be just completely over-the-top, crazy levels of inflammation and yet, there’s inflammation, but not really proportional to what just happened. And that’s because the woman’s immune system is still suppressed a little bit, let’s say.
Now during the menstrual cycle, you’ve got a huge fluctuation of hormones as the body gets ready for potentially getting pregnant, and then if that doesn’t happen, all of those hormones drop very precipitously, particularly progesterone and estrogen so that the uterine lining sheds, and that’s when most women consider that their periods starts, because that’s when bleeding starts.
But it coincides with, of course, the big drop in hormones, which is also what coincides with very often a change emotionally where that may not be the happiest time in the month of course, and it coincides with more probability of inflammation, because those hormones, progesterone and estrogen, as they’re building, they’re at the beginning of the building phase of lowering your immune response so that you can get pregnant and so that you can deliver. But when that doesn’t happen, okay, you don’t need all those hormones, they drop off. And when they drop off, they stop suppressing the immune system so the immune system gets busy again.
There may, of course, be variation in different women, because I would imagine no two are exactly alike as far as the level of specific hormone and how an individual responds to it. But on average, the progesterone and the estrogen tend to limit the inflammatory response. So when they drop very, very sharply, there’s a compensatory boost in inflammation at that point. And it may be part of what actually helps the uterus to shed its lining and get ready to start all over again later.
Clint Paddison: Okay. So you’ve covered a lot then. I’ve taken a couple of frantic notes as you’ve been talking. You’ve mentioned progesterone and estrogen. Are they the two hormones that you feel are most predominantly involved in a suppressive-like state on the inflammation in the body when once a woman is becoming or is pregnant?
Dr. Richard Matthews: Yes, I think that that would be accurate. But again, it may not. Not every woman may experience it exactly that way.
Clint Paddison: Okay. And then I’ve also been underlining some documentation that you sent to me about this as well, and I’m going to try and summarize this. It’s not what we’ve discussed so far in the call. I’m just going to summarize what you’ve sent to me in a separate document, and then try and keep it as simple as possible so that we just dip our toe into the really complex stuff for a moment, and then we may be able to just use some of the phrases to explore this just a little bit further. So let’s just see how I go here. So I’m looking for a particular picture.
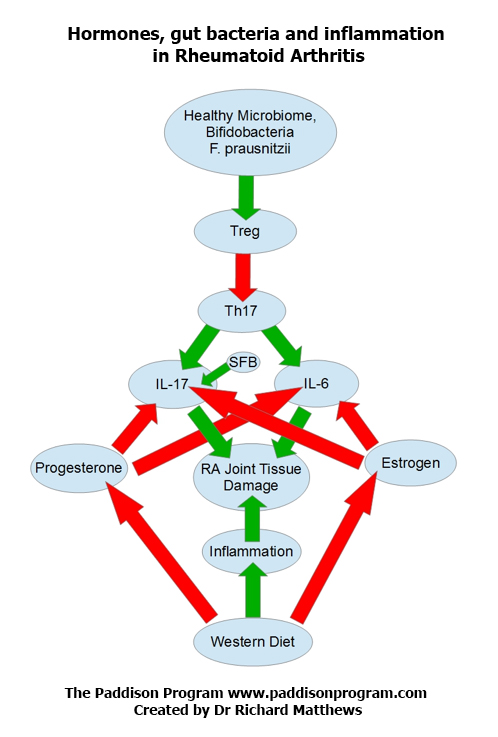
So we know that bacteria, very, very important in influencing our immune system. You’ve sent me a diagram here that says the microbiome or the collection or the environment of bacteria talk to what are called T regulatory cells, and that these T regulatory cells are called this because they regulate what are called T helper cells, and these T helper cells influence the amount of what are called cytokines. Am I so far on the right track?
Dr. Richard Matthews: Exactly on track.
Clint Paddison: Okay. And it is the cytokines that are so heavily involved in the inflammatory activity of attacking the joints. And so one step further to that, then the final step is the progesterone and estrogen actually suppress cytokines. And so the bacteria are directly influencing, through the T reg cells and the T helper cells, how many of these inflammatory molecules are being created, which are attacking the joints. And that the progesterone and the estrogen, when those levels are being elevated during pregnancy and during a period of the month for some ladies, can suppress those cytokines, and therefore, directly suppress the inflammation.
Dr. Richard Matthews: Exactly, beautifully stated, Clint. That is exactly what happens, and there are different players involved in what we call a healthy microbiome. Bifidobacteria, for example, are one of the more common ones that are known to suppress inflammatory levels through the T reg cells. And there are others that are known to make it worse, Segmented Filamentous Bacteria, for example, SFBs. They’re what get one of those cytokines, interleukin-17 actually, fired up in the first place, which early in life, you need a little bit of that, but not too much. It’s like many things. You wouldn’t want to have none of those, but if you have too many of them, you get a very imbalanced response.
There are other players there that I didn’t even include in the diagram. Prevotella copri, for example, is one organism that’s been very tied to rheumatoid arthritis, because it activates the cytokine inflammatory cascade as it’s called and sets all that in motion.
Clint Paddison: Right. Let’s just stay on that for a moment, and just can I get your pronunciation of that particular organism again?
Dr. Richard Matthews: Well, I don’t know if it’s correct, but I thought it was Prevotella copri.
Clint Paddison: That sounds fine to me. I’ve just never heard it spoken before out loud so I just want to know. It’s not a test. It’s an education to me. Prevotella copri. And if anyone does a Google search on Prevotella copri, they’ll find a bunch of fairly recent scientific work that’s been done on this, probably in the last five years or so, wouldn’t you say, Richard? It seems to have come to light in the last five years that this particular organism, a species of bacteria, is much more prevalent in people with RA than those who do not have RA, and therefore leading to the to the conclusion that maybe this acts in a negative way towards the immune system, and as you were just saying, tends to increase their cytokine activity.
I think that you mentioned to me just before we spoke on the call that simple sugars is something that the Prevotella copri may be fuelled by, and that’s why potentially some people who are following my program need to keep their sugar content very low for a longer period of time, because potentially those folks have a higher prevalence of this particular species.
Dr. Richard Matthews: That would make sense, and really, it’s becoming a recognized tactic anytime somebody wants to help their microbiome become more diverse and healthier, limiting simple carbohydrates, limiting sweets is almost…well, I can’t think of any circumstance where that’s not a good step in the right direction. We’re simply not designed or not evolved to eat sweets or simple carbs, nearly to the extent that we do. I don’t know the statistic for Australia, but in America, they say that the average American consumes 152 pounds a year of sugar and that’s just an insane amount. That’s coming up close to 2 pounds a day, which if you looked at a 5 pound bag and said, “Okay, I’m going to eat almost two-fifths of that every day,” there’s no way that could have a happy outcome but yet…
Clint Paddison: It’s insane.
Dr. Richard Matthews: And that’s factoring people like me that really don’t eat very much of it at all. So I know somebody out there’s probably over 2 pounds a day in order to come up with that average because it’s an average.
Clint Paddison: That’s right.
Dr. Richard Matthews: But that’s…at the bottom of the diagram is Western diet. And as a note, it’s always a bit sadly comical to me when news, TV shows, health shows will sometimes pronounce as some sort of announcement that, “Oh, researchers have found suggestion that the Western diet, modern diet, may play a role in some diseases,” because I’ve probably read thousands of research studies in the process of preparing the material for my book, and I continue to read them to do things like writing this chart that we’re looking at…diagram. And in the research literature, the Western diet is the research standard for creating a sick animal.
When you read the actual procedure where they describe what did we actually do, they’ll say, “Well, we started out with a standardized animal like a Wistar rat or something, and they were put on the standardized Western diet for a period of six weeks to induce Type 2 Diabetic changes, or joint arthritic changes.” And I look at that, and I think, “Wait, back up the train a little bit. What you’re just saying is that the standard way of giving the animal the disease that we want to study is to feed it what most people eat.”
And yet, we find that surprising, but it’s in the research literature. It’s been around so long that it’s the standard way to do it. There’s not even any question about it. It’s just how you come up with a sick animal. None of them say, for example, “Oh, we put the animal on a standardized macrobiotic vegetarian diet to introduce heart disease,” because you know what? It wouldn’t work. If you feed them cheeseburgers and a lot of Cokes, or a lot of sweet soft drinks, yeah, they get sick.
Clint Paddison: I love it.
Dr. Richard Matthews: Rather predictably.
Clint Paddison: I love that there’s no actual worse way or no faster way that science knows to make them sick to treat them than to give them the food that everyone’s eating.
Dr. Richard Matthews: That’s exactly it and it’s tragically humorous, because you can look coast-to-coast and except for some private schools, and maybe some schools in very well-to-do areas, what do kids…what are we feeding our children? But exactly some version of the Western diet and in America, we’ve had the government tried to step in and say, “There needs to be a vegetable.” So they add an extra packet of ketchup or something. “There’s your vegetable, kid.” But it’s nowhere near anything that science shows to be healthy.
And yet, I know, 30, 40 years down the road, people are going to be scratching their heads going, “Wow, why do we have so many sick people?” Well, what did they grow up on? Just to tie this together, we’re talking about diet right now. We started out talking about the gut bacteria and rheumatoid arthritis. But when you look at gut bacteria, after the first couple years of life, your gut bacteria are a population that’s determined by whatever survived the conditions that you put it through, which means if you starved it, it probably didn’t survive, and whatever you fed, did survive.
Any person’s gut bacteria is…it starts out with something, and then it’s what did you add to it, and what did you subtract to it? If you took a probiotic, you might have added something or fermented food. If you ate a specific diet of any kind, well, you fed one thing and you starved another. The only question is, did you feed the good guys and did you starve the ones you didn’t want so many of or are you feeding the ones that are really not serving your needs? You’re feeding the bad guys.
Clint Paddison: Yeah, I love the simplicity of how you look at that and it is so true. When we realize that we have that power, and we really are the puppeteer and the bacteria are our puppet, if we want the leg to go down representing all the bad stuff, we just don’t take any action to feed that aspect of our portfolio of bacteria, and they will eventually die away. And we have that control like a puppeteer, don’t we?
Dr. Richard Matthews: We do, but it brings to mind an image. And this is a point that really needs to be made if somebody wants to successfully work with the concept is that we’re both puppeteers; both the bacterial colony and the human host are puppeteers. If I were to draw it as a…in the form of a political cartoon, they would have a bit of a web between them, and they would each be pulling the other’s strings so that anything that either one does affects the other, and reflexively affects the one that did it.
And that’s really more the nature of the relationship. You may eat something. Okay, you boost the population of a bacteria. Well, in turn, that bacteria, when it gets its population boosted, is going to have an effect on you, and it’s going to affect what do you want to eat? What tastes good? What smells good or are you attracted to? How do you feel? What’s your energy level? And it’s a very self-serving organism. It’s going to do that in whatever way benefits it, so the ones that we call healthy are basically ones whose actions benefit us also.
Scientific American or Science magazine, there was a big article recently published that showed that a gut bacterial or a bacterial colony itself communicates within itself very much like a brain that…we’ve known about chemical messaging between bacteria for a while and quorum sensing and a few other scientific terms like that. But what they’ve found is that the bacteria can communicate with each other through ionic channels, which means they exchange electrically charged particles in a very, very similar manner to how nerves communicate with each other in a brain. And when you have trillions of the things together, the different areas get tasked with different duties, and it really does act much more like a multicellular organism or a brain.
And it has the same basic desires of any other living thing. It tries to survive and it tries to reproduce, and it will do whatever it has to do to get us things that will benefit it. So if it’s good ones, it’s like, “Oh, yeah, all of a sudden, that carrot juice is tasting pretty good.” And if it’s not very good one, it’s like, “Ah, man, I am so craving a Big Mac right now.” It’s two in the morning and you’re in the kitchen eating like leftover junk food. Yeah, your gut bacteria are definitely being the puppeteer and not in a good way.
Clint Paddison: Absolutely. I’ve got a couple of examples on that is that some people when they start the Paddison program in the first couple of days, I recommend a lot of celery and cucumber juice just a cleansing light alkalizing juice, which once you’ve had a lot is very mild. I could just drink it all the time without really giving it much thought. But if people have never had that before and they’ve been coming at it from a Western diet, people saying things like they’re almost vomiting and they’re feeling nauseous just from the smell of it so you can tell that those people are going to have the greatest benefit after they slowly work it into their bodies, and get used to it more and more, because so clearly, they are incubating lots of bacteria that do not want that kind of healthy juice inside them.
Dr. Richard Matthews: Absolutely, absolutely. And if you take somebody who’s been a health food person for years and years, and maybe they accompany a friend or something, and they stop at one of the fast food places where everything is deep-fried and junk, it doesn’t look good. It doesn’t smell good. It doesn’t even smell like food, really. And that’s such a dramatic change. It’s not really attributable to purely a personality thing, because in other things, you might look at something and say, “Oh, I know that’s not good for me, but it sure does seem attractive.”
But when it comes to big changes in diet like that, it’s really quite primal. It’s like our very wiring has been changed so that, No, that’s not good anymore.” The carrot juice, the celery juice is suddenly like, “Yeah, this stuff’s not so bad. I can do this.” That’s a wonderful, wonderful example of that type of change where you start out thinking there’s no way I’m going to get through this plan, but you make yourself do it for a few days and then it gets easier and easier, because you’re changing the whole organism that’s determining the flavour.
Clint Paddison: It does. And I think the reason that it can be suddenly putting the brakes on to the bad bacteria is because the whole thing is there’s no sugar in that drink. It’s just celery and cucumber. It’s very alkalizing. It has nothing of any benefit to anything that’s nasty in your body whatsoever. And so the complaints are very loud and clear from someone who hasn’t been eating the right foods coming up to starting the program.
Now, I wanted to just pick your brains a little bit more on our topic of hormones so that we keep it content rich still before we wrap up or get distracted on other more broad stuff as we love to do.
Dr. Richard Matthews: Oh yes.
Clint Paddison: Let’s talk about…I just want to draw reference to a wonderful, different chart that you’ve put in the documentation for me, and this chart shows the levels of progesterone and estrogen with time during pregnancy. And in this chart, it shows that when a female first falls pregnant, her progesterone and estrogen levels begin to rise, and they rise steadily and consistently, right up until the point of birth so that at birth, her levels of progesterone and estrogen are as high as they’ll ever be probably under normal conditions, including pregnancy throughout her life. And so that goes a long way to explaining why the symptoms during pregnancy continue to improve and a woman feels fabulous when she’s right up to the point of giving birth and then I love your word precipitously. It’s just such a fabulous word, precipitously.
Dr. Richard Matthews: Precipitously.
Clint Paddison: Precipitously fall away after childbirth, and so suddenly it’s like stopping steroid treatment or it’s suddenly just coming off all your medications, but your medications were natural pain reduction via progesterone and estrogen, which were suppressing the cytokine attacking the joints. And so it’s quite a dramatic and quite fascinating phenomenon that occurs right at childbirth that as those hormones fall away off the edge of the cliff, all things are about to present themselves as painful again once those hormones have dropped back down.
Dr. Richard Matthews: Absolutely. Again, it makes sense when you consider the process that is involved in childbirth. There are emotional consequences as well, because right up to the last week or two before childbirth, it’s quite common for women to really contemplate, “Wow, can I do this?” Up till the last minute and yet, have such courage to actually go through with it.
I jokingly say that if childbirth were up to men, we’d probably be extinct as a species, because we’d never agree to do it a second time, and that just doesn’t work when you play the numbers with two people having one baby. We’d be extinct. So there’s an element of, I don’t know, optimism or courage or perhaps even a dampening of anxiety and dampening of potential depression, a bit of a high perhaps when it’s time for childbirth. And I really think that that is a part of what makes it possible for a woman to even do it.
But yes, when all of those drop precipitously after childbirth, quite logically, there’s also an emotional crash, postpartum depression, which happens to a varying extent with different women. Some, it’s really not so bad and some, it’s quite devastating and debilitating, even dangerously so. Again, if men had to have that much variation in hormone, oh my God, it would wreck us and women really quite courageously manage to navigate through this.
But when you look at that big a drop in hormones, looking at the chart, it looks like some of the roller coasters that I’ve written that I love and my wife would absolutely hate, because you go up and up and up and then you go over the top corner and then just straight down. And that’s how every chart that looks at hormone levels during pregnancy and delivery depicts your progesterone and estrogen just turf right after the birth. And if it were a drug as you say and you stopped cold turkey, there’s no doubt you would have a massive rebound inflammation event happening and I feel that is what happens with a lot of people.
Now in the grand scheme of actual childbirth, inflammation of course is not completely a negative event. It’s part of how the body moves needed materials, circulation, spare parts, if you will, to a damaged area, so any structural damage that happens, overstretching of muscles, any little tears or anything, inflammation does help heal that.
But again, the body is timing it perfectly so that right immediately when it’s really happening, no there’s not that much inflammation but then the inflammation is permitted to start coming back after all those hormones drop. And it has to probably for the healing to happen after that, but unfortunately for RA sufferers, that also brings a return of inflammation in other ways that are not so good.
Clint Paddison: Yeah, however, not that there really is a however, because that pain obviously is so debilitating and painful, and we wish it wasn’t the case, but at least I think that anyone listening to this who’s been through this will be nodding their head and be grateful of an understanding of this finally, because if you do a search for it in the literature, it’s not really clear cut as to what’s causing this, which is why I wanted to reach out to you and help me with this, because it was quite difficult and you’ve really helped make this a lot more clear.
I know that we’ve tried to keep it more on the simple side of things and that I’ve not asked you specifically to go into all the detail that I know that you could on this. So I think that we’ve dipped our toe in it as I said earlier, and we’ve got a good overview. And we know that the hormones during pregnancy are suppressing the cytokines which are the inflammatory molecules that are attacking the synovial tissue. And then when pregnancy stops, the hormones which are at their highest elevation right up till birth then fall back down to normal precipitously. And as a result, all of the pain is no longer being suppressed by the hormones, and so we’re exposed again to the real situation.
And the challenge for women during pregnancy is even greater in as much as couple of other reasons. One is [inaudible 00:40:40] exercise to the extent that I like people, I like clients to exercise to when they have RA. I see exercise as 40% of the equation when trying to get well with RA just because the importance of moving the joints and getting a lot of aerobic activity through the body. So not being able to exercise means that their overall cardiovascular, lymphatic health, all of that is not as good as when they are not pregnant.
And secondly during the pregnancy, is I don’t want people to be following the type of elimination, reintroduction process that works so well for other people following the Paddison program, because I want the pregnant mom to get a really, really broad, diverse range of nutrients, and adequate or more than adequate amount of the caloric needs for their growing child and themselves. The program wasn’t designed from an elimination point of view for a pregnant woman.
Dr. Richard Matthews: Right.
Clint Paddison: And so what tends to happen is that you’ve got those three things then happening after childbirth. You haven’t been able to exercise as much. You haven’t been inclined to, and it wasn’t as easy to, and you shouldn’t be expected to so your body’s not as fit and as cleansed of the circulating immune complexes as what you would be if you’re exercising a lot. You’ve been eating a much more diverse range of foods, still within a range that I recommend but not a healing range, more of a broad nutritional range. And then all your hormones fall to zero so you’ve got no protection from the inflammation and so after childbirth, you’re thinking, “Oh my God, I’ve now got a screaming little baby that needs me every second, and all my pain’s come back,” and it can be overwhelming.
Dr. Richard Matthews: I imagine so.
Clint Paddison: Hopefully this call can be of great benefit to people who are pregnant, or have been pregnant, and coming out of pregnancy and now dealing with their young child or know what to expect as well.
Dr. Richard Matthews: Just knowing that the next cycle might bring some more relief might help, just knowing that while it’s not necessarily going to stay at this low level here, that could be a benefit too.
Clint Paddison: What are your thoughts on actually supplementing the hormones? Is it something that can be done?
Dr. Richard Matthews: It’s definitely something that can be done. It’s a contentious subject with a lot of physicians. I’ll put some thoughts out there. Of course, the biggest debate, if you will, there’s a whole group that says that bioidentical hormones are the only way to go and are far better. And there’s the rest of the profession medically that says that there’s no difference and that’s just unsubstantiated thought.
But yet, if you actually look up what these synthetic hormones are, for example, birth control pills typically are designed to simulate pregnancy to prevent pregnancy, because a woman can’t get pregnant when she is pregnant or at least that’s how it’s supposed to work with very few exceptions. So there’s something that’s like progesterone and something that’s like estrogen in birth control, but as in many things, just like, almost like isn’t really quite the same as exactly. So it’s not really progesterone, it’s a group of chemicals that are called progestins, because they’re like progesterone. They activate progesterone receptors.
But in fact, they’re not the same thing at all. If you look at the actual chemicals, they have a completely different effect. I had a page that I had pulled up on that, but it has disappeared. If you look…just even look at the Wikipedia entry for progestin with an “I-N,” you’ll see that there are six or eight different chemicals that are essentially different drug companies’ version of progestin, and it’s a slightly different chemical. All of them have in common the fact that they don’t activate only progesterone receptors, meaning that instead of a sniper rifle, you’ve got something that’s spraying buckshot out there.
And yeah, you might hit what you’re aiming to hit, but you’re probably going to hit a few other things too as collateral damage. whereas the progesterone that a woman’s body produces or bioidentical progesterone that is the same exact molecule is going to only react with a progesterone receptor and have the range of effects that the naturally produced progesterone would have. When it’s affecting several other types of receptors in the body, you can get a whole range of other effects. And honestly that’s why those have side effects. We’ve got some of it.
Clint Paddison: So what you’re saying is that there is no perfect supplement for progesterone and that the supplements that are available all have a varying wide, as you say, buckshot effect, and may have some side effects and may not be that effective.
Dr. Richard Matthews: Well, actually what I would say is that seems to be the case with the pharmaceuticals, with the drugs that for example, are birth control pills. There are supplements. There are natural sources of progesterone that are true progesterone. Progesterone cannot be taken orally from what I understand, because the digestive tract breaks it down. But it can be absorbed to an extent transdermally so you can actually get it as a cream and it’s absorbed through the skin.
Strangely, one of the groups of people that has toyed with this the most are bodybuilders. My reading on this has taught me that bodybuilders who take high levels of testosterone to build big muscles often suffer from one of the side effects of too much testosterone, which is that some of it gets converted into DHT, Dihydroxy Testosterone, which causes the hair loss, and balding, and some of the effects like that. Some of it actually gets converted into estrogen and that has some rather unwanted side effects. Namely, making testicles smaller and creating breasts, gynecomastia, also known as man boobs or simply moobs in America. That is sort of the culturally accepted term for that.
And apparently the bodybuilders have figured out some time ago that the antidote for that is small doses of progesterone that blocks the conversion of excess testosterone into DHT or estrogen and/or it blocks the DHT receptors, I forget which. But in any case, it prevents some of the harmful effects of higher levels of testosterone. So it’s not like it hasn’t been used in the past, and of course there are other medical cases I’m sure where some level of progesterone is therapeutic. Men normally have some progesterone. It’s somewhat of a precursor hormone molecule a couple steps downstream from cholesterol. Hormones go through a whole cascade of production like on a production line before they get to actually what the end product is.
Clint Paddison: And one that I looked up just before we spoke about was wild yam. Wasn’t it a derivative from wild yam or something as a cream?
Dr. Richard Matthews: Yes. Yes.
Clint Paddison: So potentially, if people wanted to give this a bit of a try, I don’t know if it’s the sort of thing that they need to consult with their practitioner beforehand. But there’s a train of thought that could suggest that they may want to try and get some of this progesterone cream derived from wild yam, rub it on their skin and see whether or not it gives them some symptomatic relief? Are we off with the pixies with that, or is that something that is genuinely worth a try if someone’s in a lot of pain?
Dr. Richard Matthews: In my opinion, it’s generally worth a try because it does not carry a great deal of risk with it. Medically, the literature says, “Yes, a high enough level of progesterone does carry a risk.” It’s unclear whether what they’re really referring to is progestin or naturally produced progesterone. My official complete answer that I give to people is, the first part being legal disclaimer, “Yes, you should talk to your physician before doing that.” And the subtitle to that is, “But your physician may not really be into that, and may not have read up on it and will probably not be very interested in you doing it.”
On the other hand, there are a number of natural health physicians, naturopathic doctors, for example, and some nurse practitioners, some medical physicians, some chiropractors who have hormone balance as their own specialty, as an area of focus where they’ve learned a great deal about how to measure hormones, how to do tests to tell day-to-day, week-to-week, what’s high, what’s low and can help somebody to actually balance their hormones.
There’s some celebrities that are really outspoken about it. They’re often criticized and because they’re celebrities, it’s a bit hard to tell how much of their good looks is plastic surgery, makeup, Photoshop or actually they really do look that good at that age. I suspect that we probably see a bit of each, but there are people out there that really do this type of work with natural hormone, or bioidentical hormones, and some people may be a bit more courageous about just winging it and say, “Well, I think I’ll just try it, and be objective and see what happens.”
Clint Paddison: I think that it’s a fascinating concept, particularly, rather than say one of the heavy pharmaceutical approach is that 98% of people with a chronic autoimmune condition are engaging with. You think about if you could replicate through hormone therapy, a raise in your progesterone and your estrogen naturally, which is something that occurs naturally during pregnancy, and therefore dramatically reduces the pain in a female with rheumatoid arthritis, then it seems like a very, very rich and exciting area of research for someone to be able to replicate that level of hormones that pregnancy provides in some kind of…whether it be a skin cream or something, and how much to apply to the body, and which parts of the body are the best places to put it for most absorption and how to monitor how much is being absorbed.
I can understand the appeal in someone wanting to explore those paths. The one thing I would say though is that this is still an attempt to try and circumvent the real solution to the problem here, which is going right back to the top of our discussion, and that if you can get your microbiome right, then these cytokines won’t be activated as much to attack the synovial tissue, and therefore, you won’t be having to try all these therapies to try and reduce the amount of cytokines, because they simply won’t be as active in engaging and attacking your body so it all comes back to the microbiome.
And just before we wrap up, just in case anyone has listened to this and they’re thinking, “Wow, I’m going to rush out and try the pill,” because that could be a way of simulating the pregnancy situation, may be getting my hormone levels up and therefore getting some pain relief.” To the contrary, I’ve actually found this one particular client that I work with inside our forum who was doing fabulously on the Paddison program, and then, the only change made was to get onto the pill for reasons, family reasons, and then that intervention alone with no other change caused her to have a dramatic worsening of RA symptoms.
And then after I put it to her that it could quite possibly be the pill, and she actually suspected too since nothing else had changed, a month after coming off it again, all of her worsening dissipated to get back to where she was before she went on the pill. So I just want to tell that story, which is a very recent story, something that’s only happened in the last four weeks. She’s only just reporting in the last week or two how much better she is now that she’s come off the pill, because I just don’t want people to misinterpret something that we discussed about 10 minutes ago. What are your thoughts on that before we wrap up?
Dr. Richard Matthews: Well, my thoughts on that are that anybody who wants to use some of this information really should listen to the entire podcast from beginning to end, and not try to pick something somewhat out of context. For example, we’ve talked about how progesterone helps to reduce the cytokine cascade and the inflammation of RA. But later on, we did discuss the progestins and estradiol that are in birth control pills are not exactly the same substance, and that is likely why they don’t have exactly the same effect. They’re much, in a way, harsher to the system because the goal is to fool your system into not ovulating so you can’t get pregnant. And while they may be effective at that, they can cause a variety of other imbalances.
And unfortunately, really, that seems to be a recurrent theme whenever you resort to pharmaceuticals. If you look at the side effects of boosting your microbiome and reducing your stress, and all of these interventions that we talk about to have gut bacteria become healthier, and then you compare that with a list of side effects of one of the biologic drugs that’s commonly prescribed for RA without much of a second thought. Look at the list of side effects; they’re up to and including death. I mean, they’re horrible.
We joke about it here in America, because the first 5 to 10 seconds of the commercial is, “Oh, we have this new drug for such and such condition.” And then there’s 20 or 30 seconds of all of the ways that it might kill you. And then the last two or three seconds are, “Talk to your doctor about so-and-so.” And you look at the commercial and think, “Oh my God, who would buy that product?” But people do.
When you compare that with, okay, what are the worst things that could really happen if you do all these natural interventions, maybe including some natural progesterone, you’re not even in the same ballpark as far as the amount of damage you can cause, but I understand there are some people with RA that may be so severe that they need to do that, perhaps just to buy time to learn what to do next. So I’m not being judgmental in saying that. People do what they have to do, but I think it’s important to really try to objectively evaluate the long-term choices and see…look at your program, okay, it helps RA. But it’s probably also going to help prevent heart disease, lower blood pressure and do a lot of other good things, because they’re intertwined. You’re lowering inflammation. You’re restoring gut bacteria. You’re restoring a balance of function so the body doesn’t try to damage itself with the immune system. It’s a great thing. It’s a wonderful way to do it.
Clint Paddison: Yeah, that’s right. But when it comes to…people like to purchase or to engage with a product that speaks directly to their symptom. And what made me laugh is here in Australia, the Vitamin D…I’m giving probably not the ideal example. Let me jump back onto this particular example is that people will question me constantly. I’ll probably get an email every other day. “Does your program work for psoriatic arthritis?”
As far as I’m concerned, they’re virtually the same underlying cause as rheumatoid arthritis, but the uptake is just so small compared to rheumatoid just because I don’t have the word rheumatoid…sorry…just doesn’t have the word psoriatic on the title even though all the explanations, all the podcast, all talk about healing the gut and the external symptoms being just symptoms of what’s going on from the inside.
Anyway, so yeah, people just want to only consider something based on the description on the label so to speak, but yes, this program has helped people get off their puffers after having asthma for all of their adult lives, psoriatic arthritis of course, lupus, ankylosing spondylitis, you name it and that’s just the autoimmune stuff, let alone the stuff like type 2 diabetes. People have been able to easily…type 2 diabetes as you know is much easier to resolve than one of those autoimmunes and become heart attack-proof. What else do you want? What else do you want?
Dr. Richard Matthews: That’s wonderful. Yeah, that’s great.
Clint Paddison: Now, the last thing is we’ve got your contact details. I’m going to grab them from a previous podcast, and put up some links to your blog and also to your book. Do you have a new book that’s come out? Am I right in recalling you mentioned something about that? A new book?
Dr. Richard Matthews: I did mention something, but new book is not finished yet. The next book is really going to be, in a way, a simplified version of “The Symbiont Factor” that does not go into quite so many molecular pathways and individual organisms but goes into how do you figure out how to troubleshoot your system, understanding what tests to do or in what order or what they mean, the importance of diet, availability of different programs.
I’ll probably mention your program, for example, because honestly, a lot of people need to have something that’s spelled out. What do I need to do? What do I need to not do? And it works well. But it’s a way of saying, “Okay, now we’ve exposed all this new science about the importance of the microbiome and the role of all these vital Symbiont organisms in human health and function, how does that apply to me? How do I know if I’m imbalanced? How would I recognize it? What are the symptoms?”
I’m going to have questionnaires and quizzes that people can go through, and look at their responses and say, “Oh, wow. I hadn’t really thought that that had something to do with this, but they all kind of point in the same direction.” I’m going to go through perhaps even as specific as what lab tests are available from which labs to understand the testing options, which ones need to be done through physicians, which ones can be done either individually or under the justification of what’s now called Citizen Science where you sort of participate in the science, and in exchange for that, you get valuable data that you can use to hack your body as it were, and figure out how to improve your microbiome.
Clint Paddison: I’ve seen that through uBiome. They’re doing that, aren’t they?
Dr. Richard Matthews: Yes. Yes. That’s a good example of it, yes.
Clint Paddison: Yeah, a few of our community forum members are having that done right at the moment, waiting on their little sample results to be sent back.
Dr. Richard Matthews: Right. And uBiome gives a good result, but they don’t really…it’s not their stated purpose to give therapeutic recommendations afterward. One of the things that I do is to go through a uBiome result, and look for patterns or look for organisms, research the organisms and the patterns that are there and correlate that with what’s going wrong with the actual patient. What are their chief complaints? What’s their functional profile? And make recommended changes based on that. That’s what the next book is about.
Clint Paddison: That’s excellent. Well, I know that our…my clients and the listeners of this program would be very interested in that. I know we’ve had a lot of people tell us how great your book is, and I’m glad that we’ve formed this ongoing relationship, because I really like getting your input, and it’s just so valuable.
Dr. Richard Matthews: Thank you.
Clint Paddison: We could talk all day. I think we’ve gone longer than ever before, which we talked about beforehand, we’d try and keep it a bit shorter.
Dr. Richard Matthews: There’s just so much to talk about it. It’s so much fun.
Clint Paddison: So much to talk about, and luckily you’ve got a wonderful radio voice that people can enjoy listening to.
Dr. Richard Matthews: Well, thank you.
Clint Paddison: Let’s wrap it up there. Thank you once again. I really appreciate it. So until we talk again, Richard Matthews, you’ve been so helpful. And I hope that the listeners have got a lot out of this episode.
Dr. Richard Matthews: Thank you so much, Clint. It’s been my pleasure and keep up the great work.
SHOW NOTES:
Richard’s Symbiont Factor is here
Clint’s Paddison Program for Rheumatoid Arthritis is here